Exenatide
 | |
| Clinical data | |
|---|---|
| Trade names | Byetta, Bydureon |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a605034 |
| Pregnancy category |
|
| Routes of administration | subcutaneous injection |
| ATC code | A10BX04 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | N/A |
| Metabolism | proteolysis |
| Biological half-life | 2.4 h |
| Excretion | renal/proteolysis |
| Identifiers | |
| CAS Number |
141732-76-5 |
| IUPHAR/BPS | 1135 |
| DrugBank |
DB01276 |
| UNII |
9P1872D4OL |
| KEGG |
D04121 |
| ECHA InfoCard | 100.212.123 |
| Chemical and physical data | |
| Formula | C184H282N50O60S |
| Molar mass | 4186.6 g/mol |
| | |
Exenatide (![]() i/ɛɡzˈɛnətaɪd/, INN, marketed as Byetta, Bydureon) is a glucagon-like peptide-1 agonist (GLP-1 agonist) medication, belonging to the group of incretin mimetics, approved in April 2005 for the treatment of diabetes mellitus type 2. Exenatide in its Byetta form is administered as a subcutaneous injection (under the skin) of the abdomen, thigh, or arm, any time within the 60 minutes before the first and last meal of the day.[1] A once-weekly injection has been approved as of January 27, 2012 under the trademark Bydureon.[2] It is manufactured by Amylin Pharmaceuticals and commercialized by AstraZeneca.
i/ɛɡzˈɛnətaɪd/, INN, marketed as Byetta, Bydureon) is a glucagon-like peptide-1 agonist (GLP-1 agonist) medication, belonging to the group of incretin mimetics, approved in April 2005 for the treatment of diabetes mellitus type 2. Exenatide in its Byetta form is administered as a subcutaneous injection (under the skin) of the abdomen, thigh, or arm, any time within the 60 minutes before the first and last meal of the day.[1] A once-weekly injection has been approved as of January 27, 2012 under the trademark Bydureon.[2] It is manufactured by Amylin Pharmaceuticals and commercialized by AstraZeneca.
Chemistry and pharmacology
Exenatide is a synthetic version of exendin-4, a hormone found in the saliva of the Gila monster that was first isolated by John Eng MD in 1992 while working at the Veterans Administration Medical Center in the Bronx, New York. It displays biological properties similar to human glucagon-like peptide-1 (GLP-1), a regulator of glucose metabolism and insulin secretion. According to the package insert, exenatide enhances glucose-dependent insulin secretion by the pancreatic beta-cell, suppresses inappropriately elevated glucagon secretion, and slows gastric emptying, although the mechanism of action is still under study.
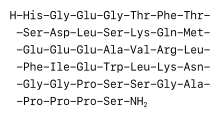
Exenatide is a 39-amino-acid peptide, an insulin secretagogue, with glucoregulatory effects. Exenatide was approved by the FDA on April 28, 2005 for patients whose diabetes was not well-controlled on other oral medication.[3] The medication is injected subcutaneously twice per day using a filled pen-like device (Byetta), or on a weekly basis with either a pen-like device or conventional syringe (Bydureon). The abdomen is a common injection site, after the area is cleaned with an alcohol pad. A new pen must first be tested to see if the medicine is flowing.
The incretin hormones GLP-1 and glucose-dependent insulinotropic peptide (GIP) are produced by the L and K endocrine cells of the intestine following ingestion of food. GLP-1 and GIP stimulate insulin secretion from the beta cells of the islets of Langerhans in the pancreas. Only GLP-1 causes insulin secretion in the diabetic state; however, GLP-1 itself is ineffective as a clinical treatment for diabetes as it has a very short half-life in vivo. Exenatide bears a 50% amino acid homology to GLP-1 and it has a longer half-life in vivo. Thus, it was tested for its ability to stimulate insulin secretion and lower blood glucose in mammals, and was found to be effective in the diabetic state. In studies on rodents, it has also been shown to increase the number of beta cells in the pancreas.
Commercially, exenatide is produced by direct chemical synthesis. Historically, exenatide was discovered as Exendin-4, a protein naturally secreted in the saliva and concentrated in the tail of the Gila monster. Exendin-4 shares extensive homology and function with mammalian GLP-1, but has a therapeutic advantage in its resistance to degradation by DPP-IV (which breaks down GLP-1 in mammals) therefore allowing for a longer pharmacological half life. The biochemical characteristics of Exendin-4 enabled consideration and development of exenatide as a diabetes mellitus treatment strategy. Given this history, exenatide is sometimes referred to as "lizard spit". Subsequent clinical testing led to the discovery of the also desirable glucagon and appetite-suppressant effects.
In its twice daily Byetta form, exenatide raises insulin levels quickly (within about ten minutes of administration) with the insulin levels subsiding substantially over the next hour or two. A dose taken after meals has a much smaller effect on blood sugar than one taken beforehand. The effects on blood sugar diminish after six to eight hours.[1] In its Byetta form, the medicine is available in two doses: 5 mcg. and 10 mcg. Treatment often begins with the 5 mcg. dosage, which is increased if adverse effects are not significant.[4] Its once weekly Bydureon form is unaffected by the time between the injection and when meals are taken. Bydureon has the advantage of providing 24‑hour coverage for blood sugar lowering, while Byetta has the advantage of providing better control of the blood sugar spike that occurs right after eating. Per the FDA label for Bydureon, Bydureon lowers HbA1c blood sugar by an average of 1.6%, while Byetta lowers it by an average of 0.9%. Both Byetta and Bydureon have similar weight loss benefits. Per the FDA approved Bydureon label, the levels of nausea are lower for Bydureon patients than for Byetta patients.
According to the manufacturer, the autoinjector must be stored in a refrigerator between 2 °C (36 °F) and 8 °C (46 °F) before first use, and then at a temperature between 2 °C (36 °F) and 25 °C (77 °F). In hot weather, therefore, they should be refrigerated.[5] Pens contain sixty doses designed to be used twice a day for 30 days.
Exenatide received US Patent 5,424,286 which was filed May 24, 1993.
Mechanism of action
Exenatide is believed to facilitate glucose control in at least five ways:
- Exenatide augments pancreas response[6] (i.e. increases insulin secretion) in response to eating meals; the result is the release of a higher, more appropriate amount of insulin that helps lower the rise in blood sugar from eating. Once blood sugar levels decrease closer to normal values, the pancreas response to produce insulin is reduced; other drugs (like injectable insulin) are effective at lowering blood sugar, but can "overshoot" their target and cause blood sugar to become too low, resulting in the dangerous condition of hypoglycemia.
- Exenatide also suppresses pancreatic release of glucagon in response to eating, which helps stop the liver from overproducing sugar when it is unneeded, which prevents hyperglycemia (high blood sugar levels).
- Exenatide helps slow down gastric emptying and thus decreases the rate at which meal-derived glucose appears in the bloodstream.
- Exenatide has a subtle yet prolonged effect to reduce appetite, promote satiety via hypothalamic receptors (different receptors than for amylin). Most people using exenatide slowly lose weight, and generally the greatest weight loss is achieved by people who are the most overweight at the beginning of exenatide therapy. Clinical trials have demonstrated the weight reducing effect continues at the same rate through 2.25 years of continued use. When separated into weight loss quartiles, the highest 25% experience substantial weight loss, and the lowest 25% experience no loss or small weight gain.
- Exenatide reduces liver fat content. Fat accumulation in the liver or nonalcoholic fatty liver disease (NAFLD) is strongly related with several metabolic disorders, in particular low HDL cholesterol and high triglycerides, present in patients with type 2 diabetes. It became apparent that exenatide reduced liver fat in mice,[7] rat[8] and more recently in man.[9]
Recently it has been demonstrated that exenatide can reverse impaired calcium signalling in steatotic liver cells,[8] which, in turn, might be associated with proper glucose control.
In an open-label, randomized, controlled trial of 551 patients,[10] exenatide treatment for 26 weeks was associated with 2.3 kg weight loss; however, gastrointestinal symptoms were more common in the exenatide group, including nausea (57.1%), vomiting (17.4%) and diarrhea (8.5%).
Indications
Exenatide is approved "as adjunctive therapy to improve glycemic control in patients with type 2 diabetes mellitus who are taking metformin, a biguanide, or a combination of metformin and a sulfonylurea, but have not achieved adequate glycemic control." It has now been approved for use with thiazolidinediones such as pioglitazone. In 2011, Byetta was approved by the FDA for use as a substitute for mealtime insulin.
- As an adjunctive therapy, exenatide is indicated to improve glycemic control in patients with type 2 diabetes who are taking metformin, a sulfonylurea, thiazolidinediones, or a combination of metformin and sulfonylurea or thiazolidinediones, but who have not been able to achieve adequate control of blood glucose.
- Its use with insulin, meglitinides, and alpha-glucosidase inhibitors has not been studied.
- Some physicians are using exenatide as primary monotherapy, an indication approved by the FDA October 30, 2009.[11]
Note: Since the major action of this drug is to enhance the release of endogenous insulin from the pancreas, exenatide is not for use in type 1 diabetes.
Side effects
The main side effects of exenatide use are gastrointestinal in nature, including acid or sour stomach, belching, diarrhea, heartburn, indigestion, nausea, and vomiting; exenatide is therefore not meant for people with severe gastrointestinal disease. Other side effects include dizziness, headache, and feeling jittery.[4] Drug interactions listed on the package insert include delayed or reduced concentrations of lovastatin, paracetamol (acetaminophen), and digoxin, although this has not been proven to alter the effectiveness of these other medications.
In response to postmarketing reports of acute pancreatitis in patients using exenatide, the FDA added a warning to the labeling of Byetta in 2007.[12][13] In August 2008, four additional deaths from pancreatitis in users of exenatide were reported to the FDA; while no definite relationship had been established, the FDA was reportedly considering additional changes to the drug's labeling.[14] Examination of the medical records of the millions of patients part of the United Healthcare Insurance plans did not show any greater rate of pancreatitis among Byetta users than among diabetic patients on other medications. However, diabetics do have a greater incidence of pancreatitis than do non-diabetics.
It also may increase risk of sulfonylurea-induced hypoglycemia.
Additionally, the FDA has raised concerns over the lack of data to determine if the long-acting once-weekly version of exenatide (but not the twice-daily form of exenatide) may increase thyroid cancer risk. This concern comes out of observing a very small but nevertheless increased risk of thyroid cancer in rodents that was observed for another drug (liraglutide) that is in the same class as exenatide. The data available for exenatide showed less of a risk towards thyroid cancer than liraglutide, but to better quantify the risk the FDA has required Amylin to conduct additional rodent studies to better identify the thyroid issue. The approved form of the once weekly exenatide [Bydureon] has a black box warning discussing the thyroid issue. Eli Lilly has reported they have not seen a link in humans, but that it cannot be ruled out. Eli Lilly has stated the drug causes an increase in thyroid problems in rats given high doses.[15]
In March 2013, the FDA issued a Drug Safety Communication announcing investigations into incretin mimetics due to findings by academic researchers.[16] A few weeks later, the European Medicines Agency launched a similar investigation into GLP-1 agonists and DPP-4 inhibitors.[17]
Future research
Long-acting release
Preliminary test results showed that exenatide was the only diabetes drug that was able to show a reduction in morbidity when it was used as part of a treatment protocol designed to intensively lower blood sugar levels of type 2 diabetics. To more thoroughly follow up on those preliminary results, Bydureon is being tested in a Phase III clinical study program called DURATION. A cardiovascular outcomes trial (EXSCEL) has also been initiated, and will include more than 9000 patients with an estimated completion in 2017. Initial trials have shown once-weekly Bydureon provides better glycemic control than the original twice-daily injectable form, with a similar weight loss profile and lower rates of nausea.
The phase III study DURATION-1 published in 2008 showed the once weekly formulation resulted in a greater HbA1c decline and more patients reaching HbA1c targets compared to twice-daily Byetta.[18]
DURATION-2 and DURATION-3, published in 2010, showed once weekly Bydureon provided superior glycemic control and superior weight loss compared to pioglitazone (Actos), the DPP-4 inhibitor sitagliptin (Januvia) and the basal insulin glargine (Lantus).[19][20]
In 2011, the National Institute for Health and Clinical Excellence (NICE) published preliminary recommendations for the use of Bydureon injection weekly. The recommendations came in triple therapy regimens (in combination with metformin and a sulphonylurea, or metformin and a thiazolidinedione) and dual therapy regimens (in combination with metformin or a sulphonylurea).[21] A decision by NICE in January 2012 approved this recommendation, allowing the drug to be added to the National Health Service formulary.[22][23]
Gene therapies
Scientists at the National Institutes of Health in Bethesda MD and other academic institutions are developing gene therapy based administration of Exendin-4 without the need for expensive daily injections.[24]
A research group led by Hee-Sook Jun published a paper in Diabetes indicating the delivery of GLP-1 through an adenoviral vector had a significant long-term effect on diabetes.[25]
Society and Culture
Lawsuit
In August 2013, a federal judiciary panel approved the consolidation of 53 lawsuits against manufacturers of "GLP-1/DPP-4 products" before a judge in U.S. District Court in San Diego. Claims involving allegations of pancreatitis, pancreatic cancer and other side effects attributed to the use of Januvia, Janumet, Byetta and Victoza will continue to be eligible for review. The order referenced the March 2013 FDA study announcement that included the drugs exenatide (Byetta, Bydureon), liraglutide (Victoza), sitagliptin (Januvia, Janumet, Janumet XR, Juvisync), saxagliptin (Onglyza, Kombiglyze XR), alogliptin (Nesina, Kazano, Oseni), and linagliptin (Tradjenta, Jentadueto).[26]
See also
- Glucagon-like peptide-1 analogs
- Liraglutide (Victoza)
- Albiglutide
- Taspoglutide
- DPP4 inhibitors
- Incretin
References
- 1 2 US Package Insert — Draft (PDF) (PDF), Eli Lilly and Company, June 2008, archived from the original (PDF) on August 20, 2008, retrieved September 6, 2008
- ↑ Pollack, Andrew (January 28, 2012). "Diabetes Drug Injected Weekly Wins F.D.A. Approval". The New York Times. p. B4. Retrieved February 25, 2012.
- ↑ CDER Drug and Biologic Approvals for Calendar Year 2005, from the U.S. Food and Drug Administration. Accessed August 28, 2008.
- 1 2 Drugs.com Accessed September 6, 2008.
- ↑ Diabetes Monitor Accessed September 6, 2008.
- ↑ Bunck MC, Diamant M, Cornér A, Eliasson B, Malloy JL, Shaginian RM, Deng W, Kendall DM, Taskinen MR, Smith U, Yki-Järvinen H, Heine RJ (2009). "One-year treatment with exenatide improves beta-cell function, compared with insulin glargine, in metformin-treated type 2 diabetic patients: a randomized, controlled trial.". Diabetes Care. 32 (5): 762–8. doi:10.2337/dc08-1797. PMC 2671094
 . PMID 19196887.
. PMID 19196887. - ↑ Ding X, Saxena NK, Lin S, Gupta NA, Gupta N, Anania FA (2006). "Exendin-4, a glucagon-like protein-1 (GLP-1) receptor agonist, reverses hepatic steatosis in ob/ob mice.". Hepatology. 43 (1): 173–81. doi:10.1002/hep.21006. PMC 2925424. PMID 16374859.
- 1 2 Ali ES, Hua J, Wilson CH, Tallis GA, Zhou FH, Rychkov GY, Barritt GJ. "The glucagon-like peptide-1 analogue exendin-4 reverses impaired intracellular Ca2+ signalling in steatotic hepatocytes". BBA-Molecular Cell Research. doi:10.1016/j.bbamcr.2016.05.006.
- ↑ Tushuizen ME, Bunck MC, Pouwels PJ, van Waesberghe JH, Diamant M, Heine RJ (2006). "Incretin mimetics as a novel therapeutic option for hepatic steatosis.". Liver Int. 26 (8): 1015–7. doi:10.1111/j.1478-3231.2006.01315.x. PMID 16953843.
- ↑ Heine RJ, Van Gaal LF, Johns D, Mihm MJ, Widel MH, Brodows RG (2005). "Exenatide versus insulin glargine in patients with suboptimally controlled type 2 diabetes: a randomized trial.". Ann Intern Med. 143 (8): 559–69. doi:10.7326/0003-4819-143-8-200510180-00006. PMID 16230722.
- ↑ exenatide approved as primary monotherapy, as announced by Eli Lilly and Co.
- ↑ 2007 Safety Alerts for Drugs, Biologics, Medical Devices, and Dietary Supplements, from the U.S. Food and Drug Administration. Accessed August 28, 2008.
- ↑ "Byetta (exenatide) FDA warning". Retrieved 2007-10-18.
- ↑ Diabetes Drug Tied to New Deaths. New York Times. August 26, 2008; accessed August 28, 2008.
- ↑ Lilly’s Once-Weekly Byetta May Have Cancer Risk // Pharmalot. Pharmalot.com (2010-04-12). Retrieved on 2011-04-16.
- ↑ "FDA investigating reports of possible increased risk of pancreatitis and pre-cancerous findings of the pancreas from incretin mimetic drugs for type 2 diabetes". FDA. U.S. Food and Drug Administration. March 3, 2013. Retrieved 2013-03-14.
- ↑ "European Medicines Agency investigates findings on pancreatic risks with GLP-1-based therapies for type-2 diabetes". EMA. European Medicines Agency Sciences Medicines Health. March 26, 2013. Retrieved 2013-03-26.
- ↑ Drucker DJ, Buse JB, Taylor K, Kendall DM, Trautmann M, Zhuang D, Porter L (2008). "Exenatide once weekly versus twice daily for the treatment of type 2 diabetes: a randomised, open-label, non-inferiority study". Lancet. 372 (9645): 1240–50. doi:10.1016/S0140-6736(08)61206-4. PMID 18782641.
- ↑ Diamant M, Van Gaal L, Stranks S, Northrup J, Cao D, Taylor K, Trautmann M (2010). "Once weekly exenatide compared with insulin glargine titrated to target in patients with type 2 diabetes (DURATION-3): an open-label randomised trial". Lancet. 375 (9733): 2234–43. doi:10.1016/S0140-6736(10)60406-0. PMID 20609969.
- ↑ Bergenstal RM, Wysham C, Macconell L, Malloy J, Walsh B, Yan P, Wilhelm K, Malone J, Porter LE (2010). "Efficacy and safety of exenatide once weekly versus sitagliptin or pioglitazone as an adjunct to metformin for treatment of type 2 diabetes (DURATION-2): a randomised trial". Lancet. 376 (9739): 431–9. doi:10.1016/S0140-6736(10)60590-9. PMID 20580422.
- ↑ "NICE recommends long-acting exenatide for type 2 diabetes in draft guidance". Retrieved October 26, 2011.
- ↑ "UK Body Recommends Lilly, Amylin Diabetes Drug Bydureon". The Wall Street Journal. January 12, 2012. online.wsj.com. Retrieved January 15, 2012{{inconsistent citations}}
- ↑ "UK Body Recommends Eli Lilly and Company (LLY), Amylin Pharmaceuticals, Inc. (AMLN) Diabetes Drug Bydureon". BioSpace. January 13, 2012. Retrieved January 15, 2012{{inconsistent citations}}
- ↑ Baggio LL, Holland D, Wither J, Drucker DJ (2006). "Lymphocytic Infiltration and Immune Activation in Metallothionein Promoter–Exendin-4 (MT-Exendin) Transgenic Mice". Diabetes. 55 (6): 1562–1570. doi:10.2337/db05-1502. PMID 16731818.
- ↑ Lee YS, Shin S, Shigihara T, Hahm E, Liu MJ, Han J, Yoon JW, Jun HS (2007). "Glucagon-Like Peptide-1 Gene Therapy in Obese Diabetic Mice Results in Long-Term Cure of Diabetes by Improving Insulin Sensitivity and Reducing Hepatic Gluconeogenesis". Diabetes. 56 (6): 1671–1679. doi:10.2337/db06-1182. PMID 17369525.
- ↑ "IN RE: INCRETIN MIMETICS PRODUCTS LIABILITY LITIGATION" (PDF). USJP. United States Judicial Panel on Multidistric Litigation. August 26, 2013. Retrieved 2013-08-26.
External links
- Instructions
- Byetta website
- Byetta prescribing information (with clinical studies references)
- NY Times Article on Byetta
- exenatide at the US National Library of Medicine Medical Subject Headings (MeSH)
- Conference, inc graphs of results with eventide