Real ear measurement
Real ear measurement (REM, also known as insitu- or probe microphone measurement)[1] is the measurement of sound pressure level in a patient's ear canal developed when a hearing aid is worn. It is measured with the use of a silicone probe tube inserted in the canal connected to a microphone outside the ear and is done to verify that the hearing aid is providing suitable amplification for a patient's hearing loss.[2] The American Speech–Language–Hearing Association (ASHA) and American Academy of Audiology (AAA) recommend real ear measures as the preferred method of verifying the performance of hearing aids.[3][4] Used by audiologists and other hearing healthcare practitioners in the process of hearing aid fitting, real ear measures are the most reliable and efficient method for assessing the benefit provided by the amplification.[5] Measurement of the sound level in the ear canal allows the clinician to make informed judgements on audibility of sound in the ear and the effectiveness of hearing aid treatment.
The use of real ear measurement to assess the performance of hearing aids is covered in the ANSI specification Methods of Measurement of Real-Ear Performance Characteristics of Hearing Aids, ANSI S3.46-2013 (a revision of ANSI S3.46-1997).[6]
History
The first commercially produced real ear measurement available was made by Rastronics.[7] Help soon arrived. In the early 1980s, the first computerized probe-tube microphone system, the Rastronics CCI-10 (developed in Denmark by Steen Rasmussen), entered the U.S. market (Nielsen and Rasmussen, 1984). This system had a silicone tube attached to the microphone (the transmission of sound through this tube was part of the calibration process), which eliminated the need to place the microphone itself in the ear canal. By early 1985, three or four different manufactures had introduced this new type of computerized probemicrophone equipment, and this hearing aid verification procedure became part of the standard protocol for many audiology clinics.
Method
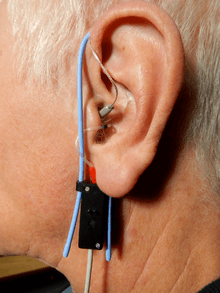
First, the clinician will examine the ear canal with the use of an otoscope to ensure no wax or other debris will interfere with the positioning of the probe tube. The probe tube is placed with the tip approximately 6 mm (1/4 inch) from the tympanic membrane. Next the hearing aid is put in place. The REM system will typically produce a test stimulus from a loudspeaker situated 12–15 inches (30–38 cm) from the patient's head and simultaneously measure the output in the ear canal to determine how much amplification the hearing aid is providing.[8]
Insertion gain
The traditional method of real ear measurement is known as insertion gain, which is the difference between the sound pressure level measured near the ear drum with a hearing aid in place, and the sound pressure level measured in the unaided ear. First a measurement is made with the probe tube in the open ear (Real Ear Unaided Response, or REUR), then a second one is made using the same test signal with the hearing aid in place and turned on (Real Ear Aided Response, or REAR). The difference between these two results is the insertion gain. This gain can be matched to targets produced by various prescriptive formula based on the patient's audiogram or individual hearing loss.[9]
Speech mapping
Speech mapping (also known as output-based measures) involves testing with a speech or speech-like signal. The hearing aid is adjusted so that the speech is amplified to the approximate middle of the patient's residual auditory area (the amplitude range between the patient's hearing threshold and upper limit of comfort) while observing a real-time spectrum display of the speech in the patient's ear canal. Many multi-channel hearing aids allow each frequency channel to be adjusted separately. The aim is to find a good compromise between intelligibility and loudness discomfort.[10] This approach to hearing aid testing is implemented in most current real ear systems and there has been a significant increase in audiologists selecting to verify using the output method.[11] Using a real speech signal to test a hearing aid has the advantage that features that may need to be disabled in other test approaches can be left active, and the effects of these features in normal use are included in the test.[12]
See also
References
- ↑ Stach, Brad (2003). Comprehensive Dictionary of Audiology (2nd ed.). Clifton Park NY: Thompson Delmar Learning. p. 167. ISBN 1-4018-4826-5.
- ↑ Valente, Michael; John E. Tecca (1994). "Chapter 5". Strategies for Selecting and Verifying Hearing Aid Fittings. NY: Thieme Medical Publishers. p. 88. ISBN 0-86577-500-1.
- ↑ ASHA Ad Hoc Committee on Hearing Aid Selection and Fitting (1998). "Guidelines for Hearing Aid Fitting for Adults". American Journal of Audiology. 7 (5–13). doi:10.1044/1059-0889.0701.05 (inactive 2015-11-26).
- ↑ Valente, Michael; Harvey Abrams; Darcy Benson; Theresa Chisolm; Dave Citron; Dennis Hampton, Angela Loavenbruck, Todd Ricketts, Helena Solodar, Robert Sweetow (2007). "Guidelines for the Audiologic Management of Adult Hearing Impairment" (PDF). American Academy of Audiology. Retrieved 3 February 2014.
- ↑ Jack Katz; Larry Medwetsky; Robert Burkard; Linda Hood (2009). "Chapter 38, Hearing Aid Fitting for Adults: Selection, Fitting, Verification, and Validation". Handbook of Clinical Audiology (6th ed.). Baltimore MD: Lippincott Williams & Wilkins. p. 858. ISBN 978-0-7817-8106-0.
- ↑ ANSI/ASA Standard S3.46-2013 "Methods of Measurement of Real-Ear Performance Characteristics of Hearing Aids," Acoustical Society of America, Melville, New York, http://acousticalsociety.org/
- ↑ Venema, Theodore (2014). "Real Ear Measures Today: Do We Truly Follow Fitting Methods?". Canadian Hearing Report. 9 (4): 7.
- ↑ Valente, Michael; John E. Tecca (1994). "5. Use of Real-Ear Measurements To Verify Hearing Aid Fittings". Strategies for Selecting and Verifying Hearing Aid Fittings. NY: Thieme Medical Publishers. pp. 93–95. ISBN 0-86577-500-1.
- ↑ Valente, Michael; George A. Gates (1994). "13. Aural Rehabilitation for Individuals with Severe and Profound Hearing Impairment: Hearing Aids, Cochlear Implants, Counseling, and Training". Strategies for Selecting and Verifying Hearing Aid Fittings. NY: Thieme Medical Publishers. p. 277. ISBN 0-86577-500-1.
- ↑ Moore, Brian C.J. (August 2006). "Speech mapping is a valuable tool for fitting and counseling patients". Hearing Journal. 59 (8): 26, 28, 30. doi:10.1097/01.HJ.0000286371.07550.5b. Retrieved 6 February 2014.
- ↑ Jack Katz; Larry Medwetsky; Robert Burkard; Linda Hood (2009). "Chapter 38, Hearing Aid Fitting for Adults: Selection, Fitting, Verification, and Validation". Handbook of Clinical Audiology (6th ed.). Baltimore MD: Lippincott Williams & Wilkins. p. 859. ISBN 978-0-7817-8106-0.
- ↑ Ross, Mark (2007). "Evaluating the Performance of a Hearing Aid in the Real-Ear". Rehabilitation Engineering Research Center on Hearing Enhancement. Gallaudet University. Retrieved 6 February 2014.