Penicillium marneffei
| Penicillium marneffei | |
|---|---|
| Scientific classification | |
| Kingdom: | Fungi |
| Phylum: | Ascomycota |
| Class: | Euascomycetes |
| Order: | Eurotiales |
| Family: | Trichocomaceae |
| Genus: | Penicillium |
| Species: | P. marneffei |
| Binomial name | |
| Penicillium marneffei Segretain | |
Penicillium species are usually regarded as unimportant in terms of causing human disease. Penicillium marneffei, discovered in 1956, is an exception. This is the only known thermally dimorphic species of Penicillium, and it can cause a lethal systemic infection (penicilliosis) with fever and anaemia similar to disseminated cryptococcosis.
Epidemiology
There is a high incidence of penicilliosis in AIDS patients in SE Asia; 10% of patients in Hong Kong get penicillosis as an AIDS-related illness. Cases of P. marneffei human infections (penicillosis) have also been reported in HIV-positive patients in Australia, Europe, Japan, the UK and the U.S.. All the patients, except one,[1] had visited Southeast Asia previously.
Discovered in bamboo rats (Rhizomys) in Vietnam,[2] it is associated with these rats and the tropical Southeast Asia area. Penicillium marneffei is endemic in Burma (Myanmar), Cambodia, Southern China, Indonesia, Laos, Malaysia, Thailand and Vietnam.
Although both the immunocompetent and the immunocompromised can be infected, it is extremely rare to find systemic infections in HIV-negative patients.
The incidence of P. marneffei is increasing as HIV spreads throughout Asia. An increase in global travel and migration means it will be of increased importance as an infection in AIDS sufferers.
Penicillium marneffei has been found in bamboo rat faeces, liver, lungs and spleen. It has been suggested that these animals are a reservoir for the fungus. It is not clear whether the rats are affected by P. marneffei or are merely asymptomatic carriers of the disease.
One study of 550 AIDS patients showed that the incidence was higher during the rainy season, which is when the rats breed but also when conditions are more favorable for production of fungal spores (conidia) that can become airborne and be inhaled by susceptible individuals.
Another study could not establish contact with bamboo rats as a risk factor, but exposure to the soil was the critical risk factor. However, soil samples failed to yield much of the fungus.
It is not known whether people get the disease by eating infected rats, or by inhaling fungi from their faeces.
There is an example of an HIV-positive physician who was infected while attending a course on tropical microbiology. He did not handle the organism, though students in the same laboratory did. It is presumed he contracted the infection by inhaling aerosol containing P. marneffei conidia. This shows that airborne infections are possible.
Clinical Presentation
Patients commonly present with symptoms and signs of infection of the reticuloendothelial system, including generalized lymphadenopathy, hepatomegaly, and splenomegaly. The respiratory system is commonly involved as well; cough, fever, dyspnea, and chest pain may be present, reflecting the probable inhalational route of acquisition. Approximately one-third of patients may also exhibit gastrointestinal symptoms, such as diarrhea.[3][4][5]
Laboratory diagnosis
The fact that Penicillium marneffei is thermally dimorphic is a relevant clue when trying to identify it. However, it should be kept in mind that other human-pathogenic fungi are thermally dimorphic as well. Cultures should be done from bone marrow, skin, blood and sputum samples.
Plating samples out onto two Sabouraud agar plates, then incubating one at 30 °C and the other at 37 °C, should result in two different morphologies. A mold-form will grow at 30 °C, and a yeast-form at 37 °C.
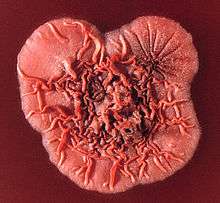
Mycelial colonies will be visible on the 30 °C plate after two days. Growth is initially fluffy and white and eventually turns green and granular after sporulation has occurred. A soluble red pigment is produced, which diffuses into the agar, causing the reverse side of the plate to appear red or pink. The periphery of the mold may appear orange-coloured, and radial sulcate folds will develop.
Under the microscope, the mold phase will look like a typical Penicillium, with hyaline, septate and branched hyphae; the conidiophores are located both laterally and terminally. Each conidiophore gives rise to three to five phialides, where chains of lemon-shaped conidia are formed.
On the 37 °C plate, the colonies grow as yeasts. These colonies can be cerebriform, convoluted, or smooth. There is a decreased production in pigment, the colonies appearing cream/light-tan/light-pink in colour. Microscopically, sausage-shaped cells are mixed with hyphae-like structures. As the culture ages, segments begin to form. The cells divide by binary fission, rather than budding. The cells are not yeast cells, but rather arthroconidia. Culturing isn't the only method of diagnosis. A skin scraping can be prepared, and stained with Wright's stain. Many intracellular and extracellular yeast cells with crosswalls are suggestive of P. marneffei infection. Smears from bone marrow aspirates may also be taken; this is regarded as the most sensitive method. These samples can be stained with the Giemsa stain. Histological examination can also be done on skin, bone marrow or lymph nodes.
The patient's history also is a diagnostic help. If they have traveled to Southeast Asia and are HIV-positive, then there is an increased risk of them having penicilliosis.
Antigen testing of urine and serum, and PCR amplification of specific nucleotide sequences have been tried, with high sensitivity and specificity. Rapid identification of penicilliosis is sought, as prompt treatment is critical. Treatment should be provided as soon as penicilliosis is suspected.
Treatment
2 weeks of amphotericin B, then 10 weeks of oral itraconazole.
Research
Sexual reproduction
P. marneffei had been assumed to reproduce exclusively by asexual means based on the highly clonal population structure of this species. However, studies by Henk et al.[6] (2012) revealed that the genes required for meiosis are present in P. marneffei. In addition, they obtained evidence for mating and genetic recombination in this species. Henk et al.[6] concluded that P. marneffei is sexually reproducing, but recombination in natural populations is most likely to occur across spatially and genetically limited distances resulting in a highly clonal population structure. It appears that sex can be maintained in this species even though very little genetic variability is produced.
References
- ↑ Lo Y, Tintelnot K, Lippert U, Hoppe T (2000). "Disseminated Penicillium marneffei infection in an African AIDS patient". Trans R Soc Trop Med Hyg. 94 (2): 187. doi:10.1016/S0035-9203(00)90271-2. PMID 10897365.
- ↑ Capponi M, Segretain G, Sureau P (1956). "Pénicillose de Rhizomys sinensis". Bull Soc Pathol Exot. 49 (3): 418–21.
- ↑ Louthrenoo, W; Thamprasert, K; Sirisanthana, T (Dec 1994). "Osteoarticular penicilliosis marneffei. A report of eight cases and review of the literature.". British journal of rheumatology. 33 (12): 1145–50. doi:10.1093/rheumatology/33.12.1145. PMID 8000744.
- ↑ Duong, TA (Jul 1996). "Infection due to Penicillium marneffei, an emerging pathogen: review of 155 reported cases.". Clinical Infectious Diseases. 23 (1): 125–30. doi:10.1093/clinids/23.1.125. PMID 8816141.
- ↑ Supparatpinyo, K; Khamwan, C; Baosoung, V; Nelson, KE; Sirisanthana, T (Jul 9, 1994). "Disseminated Penicillium marneffei infection in southeast Asia.". Lancet. 344 (8915): 110–3. doi:10.1016/s0140-6736(94)91287-4. PMID 7912350.
- 1 2 Henk DA, Shahar-Golan R, Devi KR, Boyce KJ, Zhan N, Fedorova ND, Nierman WC, Hsueh PR, Yuen KY, Sieu TP, Kinh NV, Wertheim H, Baker SG, Day JN, Vanittanakom N, Bignell EM, Andrianopoulos A, Fisher MC (2012). "Clonality despite sex: the evolution of host-associated sexual neighborhoods in the pathogenic fungus Penicillium marneffei". PLoS Pathog. 8 (10): e1002851. doi:10.1371/journal.ppat.1002851. PMC 3464222
 . PMID 23055919.
. PMID 23055919.
Further reading
- Vanittanakom N, Cooper CR Jr, Fisher MC, Sirisanthana T (2006). "Penicillium marneffei infection and recent advances in the epidemiology and molecular biology aspects". Clin Microbiol Rev. 19 (1): 95–110. doi:10.1128/CMR.19.1.95-110.2006. PMC 1360277. PMID 16418525.
